Coronavirus (COVID-19): modelling the epidemic (issue no. 72)
Latest findings in modelling the COVID-19 epidemic in Scotland, both in terms of the spread of the disease through the population (epidemiological modelling) and of the demands it will place on the system, for example in terms of health care requirement.
Coronavirus (COVID-19): modelling the epidemic in Scotland (Issue No. 72)
Background
This is a report on the Scottish Government modelling of the spread and level of Covid-19. This updates the previous publication on modelling of Covid-19 in Scotland published on 30th September 2021. The estimates in this document help the Scottish Government, the health service and the wider public sector plan and put into place what is needed to keep us safe and treat people who have the virus.
This edition of the research findings focuses on the epidemic as a whole, looking at estimates of R, growth rate and incidence as well as local measures of change in the epidemic.
In Scotland, the modelled estimate for R is between 0.7 and 1.0, with the growth rate between -5% and -1%.
Key Points
- The reproduction rate R in Scotland is currently estimated as being between 0.7 and 1.0, as of 21st September. This is unchanged since last week.
- The number of new daily infections for Scotland is estimated as being between 103 and 155, per 100,000 people. The lower and upper limits have decreased since last week.
- The growth rate for Scotland is currently estimated as between -5% and -1%.
- New research from the EAVE II group identified certain groups at higher risk of a serious Covid-19 infection. These severe Covid outcomes were associated with older age, comorbidities, hospitalisation in the previous 4 weeks, high-risk occupations (based on taking 10 or more tests weekly vs none), care home residence, living in a deprived area, being male and being an ex-smoker.
- The EAVE II study also found people with a history of the following conditions were at increased risk of being admitted to hospital or dying due to Covid-19, even after having at least one vaccine: asthma, chronic kidney disease, heart failure, type 2 diabetes, dementia and coronary heart disease.
- Hospital and ICU occupancies have plateaued, and are falling slowly. There continues to be uncertainty over hospital occupancy and intensive care in the next three weeks.
- Modelled rates of positive tests per 100K using data to 4th October indicate that, for the week commencing 17th October 2021, there are 29 local authorities which are expected to exceed 50 cases per 100k with at least 75% probability.
- There are no local authorities which are expected to exceed 300 cases per 100k with at least 75% probability.
- Nationwide, the levels of Covid-19 in wastewater (WW) following the September peak appeared to plateau this week, with significant variability in levels from observation to observation. In contrast, case rates continue to decline, though both WW and cases are comparable with the July 2021 peak.
- Modelling of long Covid gives estimates that on 24th October 2021 between 1.0% and 2.3% of the population are projected to experience symptoms for 12 weeks or more after their first suspected Covid infection in Scotland. The upper limit of the estimate is higher than last week.
Recent cases
Figure 1 shows the number of Covid-19 cases reported in Scotland between July and October 2021[1]. The vertical dashed lines indicate the cut off points for each of the modelling inputs; after these dates, the number of cases is not incorporated into the outputs.

R, growth rate and incidence are as of 21st September (dashed line 1). The medium term projections by the Scottish Government of infections, hospitalisations and ICU beds, the modelled rates of positive tests per 100k, the long Covid analysis, and the wastewater analysis use data to 4th October (dashed line 2).
Overview of Scottish Government Modelling
Modelling outputs are provided here on the current epidemic in Scotland as a whole, based on a range of methods. Because it takes a little over three weeks on average for a person who catches Covid-19 to show symptoms, become sick, and either die or recover, there is a time lag in what our model can tell us about any re-emergence of the epidemic and where in Scotland this might occur.
However modelling of Covid-19 deaths is an important measure of where Scotland lies in its epidemic as a whole. In addition, the modelling groups that feed into the UK Health Security Agency (UKHSA) consensus use a range of other data along with deaths in their estimates of R and the growth rate. These outputs are provided in this research findings. The type of data used in each model to estimate R is highlighted in Figure 2.
We use the Scottish Contact Survey (SCS) to inform a modelling technique based on the number of contacts between people. Over time, a greater proportion of the population will be vaccinated. This is likely to impact contact patterns and will become a greater part of the analysis going forwards.
The logistical model utilises results from the epidemiological modelling, principally the number of new infections. The results are split down by age group, and the model is used to give a projection of the number of people that will go to hospital, and potentially to ICU. This will continue to be based on both what we know about how different age groups are affected by the disease and the vaccination rate for those groups to estimate the proportion of cases that will require hospital, and the length of time people that people will stay there.
What the modelling tells us about the epidemic as a whole
The R value and growth rates are estimated by several independent modelling groups based in universities, Public Health England (PHE) and the Joint Biosecurity Centre. Estimates are considered, discussed and combined at the Epidemiology Modelling Review Group (EMRG), which sits within the UKHSA.
UKHSA's consensus view across these methods, was that the value of R as at 21st September[2] in Scotland was between 0.7 and 1.0 (see Figure 2)[3].
R is an indicator that lags by two to three weeks and therefore should not be expected to reflect recent fluctuations.
This week the Scottish Government presented two outputs to EMRG. The first uses confirmed cases, as published by Public Health Scotland (PHS), and deaths from National Records Scotland (NRS). The second uses instead wastewater data to estimate the number of cases, and deaths from NRS. Both outputs are shown in Figures 2 and 3.
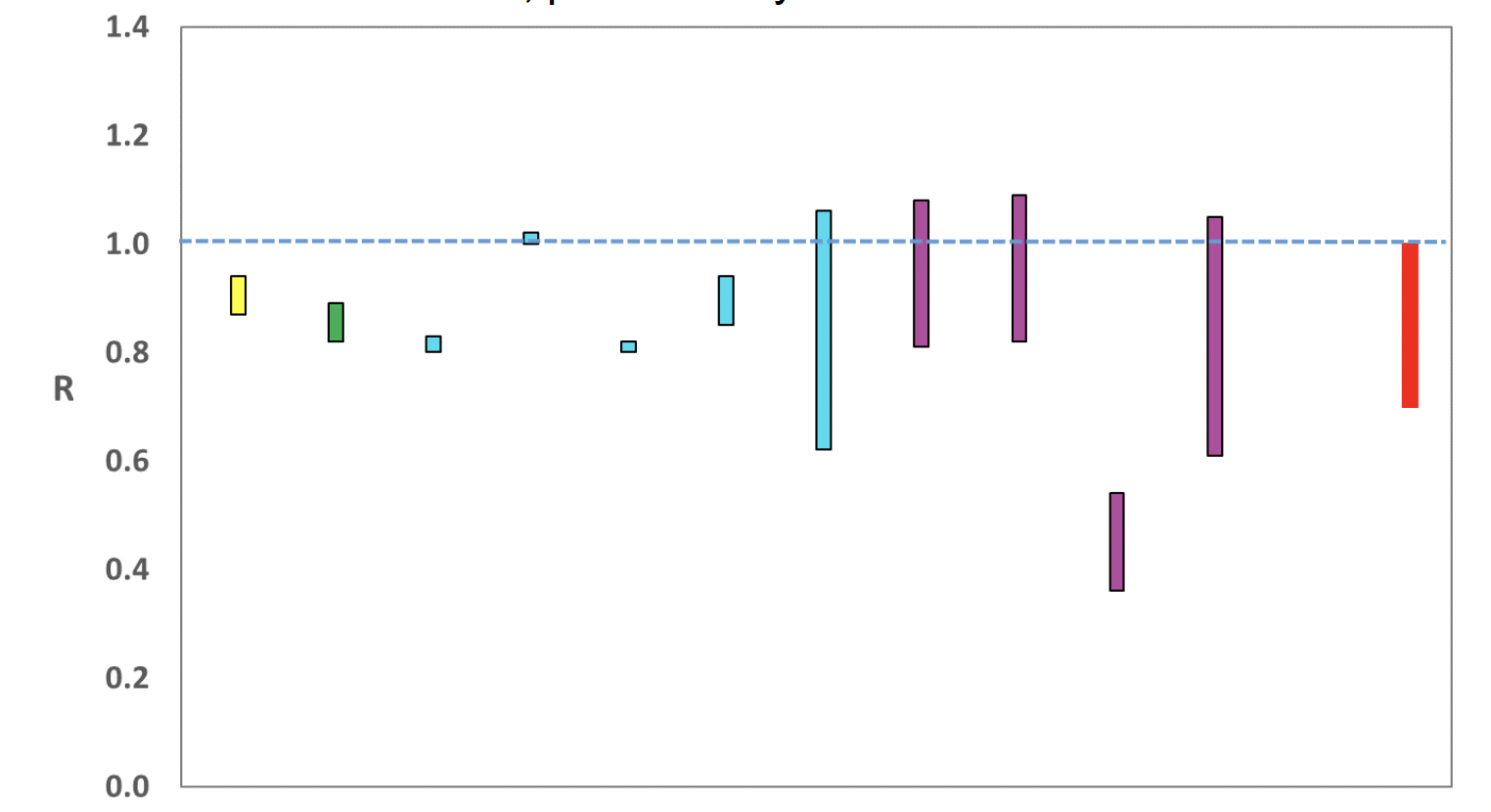
Source: EMRG
The various groups which report to the EMRG use different sources of data in their models to produce estimates of incidence (Figure 3). UKHSA's consensus view across these methods, as at 21st September, was that the incidence of new daily infections in Scotland was between 103 and 155 new infections per 100,000. This equates to between 5,600 and 8,500 people becoming infected each day in Scotland. The lower and upper limits have decreased since last week.

Source: EMRG
The consensus from UKHSA for this week is that the growth rate in Scotland is between -5% and -1% per day as at 21st September. The lower limit has decreased since last week.
New research by the EAVE II group published in The Lancet Respiratory Medicine[5] looks at the number of people in Scotland who have died from or been admitted to hospital with Covid-19 after at least one vaccine dose.
The Covid-19 vaccination programme started on 8th December 2020 in Scotland with the Pfizer-BioNTech (BNT162b2) vaccine. Vaccination clinics and GPs started to give the Oxford-AstraZeneca (ChAdOx1) vaccine on 4th January 2021, after it was approved by the Medicines and Healthcare products Regulatory Agency (MHRA). In Scotland, 2.57 million adults (62% of adult population) were given the first dose of a Covid-19 vaccine between 8th December 2020 and 18th April 2021. Two-thirds of this group had the Oxford Astra-Zeneca vaccine and one‑third had the Pfizer-BioNTech vaccine.
Why was this study carried out?
Looking carefully at the number and type of people who develop severe Covid-19 even after being vaccinated can provide important information for healthcare decisions, including:
- how to prioritise second vaccine and possibly booster doses;
- updating advice on which people should shield; and
- predicting future pressures on the National Health Service.
Researchers wanted to look at how many people in Scotland have been admitted to hospital or died of Covid-19 after at least one vaccine dose, and whether particular groups are at higher risk than others.
Their analysis is the first study on a national scale to do this. They used the EAVE II database to carry out the research.
What definitions did they use?
The EAVE II group looked at who was admitted to hospital or died because of Covid-19. They started their analysis from 14 days after each person received their first vaccination, to allow for the time needed to build up immune protection after vaccination.
Covid-19 hospital admissions are defined here as anyone admitted to hospital within 0-14 days of a positive polymerase chain reaction (PCR) test, or with Covid-19 recorded as the reason they were admitted. This also includes anyone admitted to hospital for a non-Covid reason who had a positive PCR test during their time in hospital.
In their definition of Covid-19 deaths, the group included all those who died within 28 days of a positive PCR test, or with Covid-19 listed as the main cause of death on their death certificate.
What did the EAVE II group find?
They found that between 8th December 2020 and 18th April 2021, less than one in 2000 vaccinated people in Scotland had a serious Covid-19 event[6], despite high background levels of infection at the time.
Of the 2.57 million adults given the first dose of their vaccine, 883 people were admitted to hospital with Covid-19. In the same period, 541 people died of Covid-19.
Nearly 700,000 people (27% of those included in the study) had their second vaccine during this time period. Of these, 39 (0.006%) suffered one of these serious events.
Finally, the group found that having had a Covid-19 infection before being vaccinated reduced a person's risk of serious Covid-19 disease after vaccination. This was the case for both types of vaccine studied.
Which groups are at higher risk of serious Covid-19 even after being vaccinated?
To find any high-risk groups, they included in their analysis: age, sex at birth, Covid-19 and recent hospitalisation history, relevant underlying health conditions, level of deprivation by postcode, smoking status, urban/rural residence, and time since first vaccination.
They looked at risk for the Pfizer-BioNTech and Oxford-AstraZeneca vaccines combined and individually. The following groups were at higher risk of serious Covid-19 even after vaccination, listed in order with the highest first:
1. Being older (over 80s vs 18-64 years)
2. Having multiple underlying health conditions (5+ compared to none)
3. Being admitted to hospital in the previous four weeks
4. Having a high-risk occupation (based on taking 10 or more tests weekly vs none)
5. Being a care home resident
6. Living in a deprived area
7. Being male
8. Being an ex-smoker.
The risks listed above range from roughly five times higher for age, to only slightly higher for ex-smokers compared to non-smokers. All of these conditions, except for smoking history, are also linked to higher risk of serious Covid-19 in unvaccinated people.
Taking into account age, sex and level of social deprivation, the group found people with a history of the following conditions were at increased risk of being admitted to hospital or dying due to Covid-19, even after having at least one vaccine:
- Asthma
- Chronic kidney disease
- Heart failure
- Type 2 diabetes
- Dementia
- Coronary heart disease.
Although people in the groups shown above are at higher risk of serious Covid-19 events, the total number of serious events is still low in people who have had two vaccine doses. These data may also help to prioritise people at higher risk for booster vaccines.
What the modelling tells us about estimated infections as well as Hospital and ICU bed demand
The Scottish Government assesses the impact of Covid-19 on the NHS in the next few weeks in terms of estimated number of infections. Figure 4 shows three projections over the three weeks to 24th October.
'Worse' assumes a rise in transmission similar to that seen in June and August. 'Central' assumes that infections will plateau at the current level. 'Better' assumes that infections will continue to fall[7]. After excluding the Worse scenario in recent weeks, we have included it again this week in response to Covid-19 in wastewater, where the levels of Covid-19 following the September peak has plateaued with significant variability in levels from observation to observation.
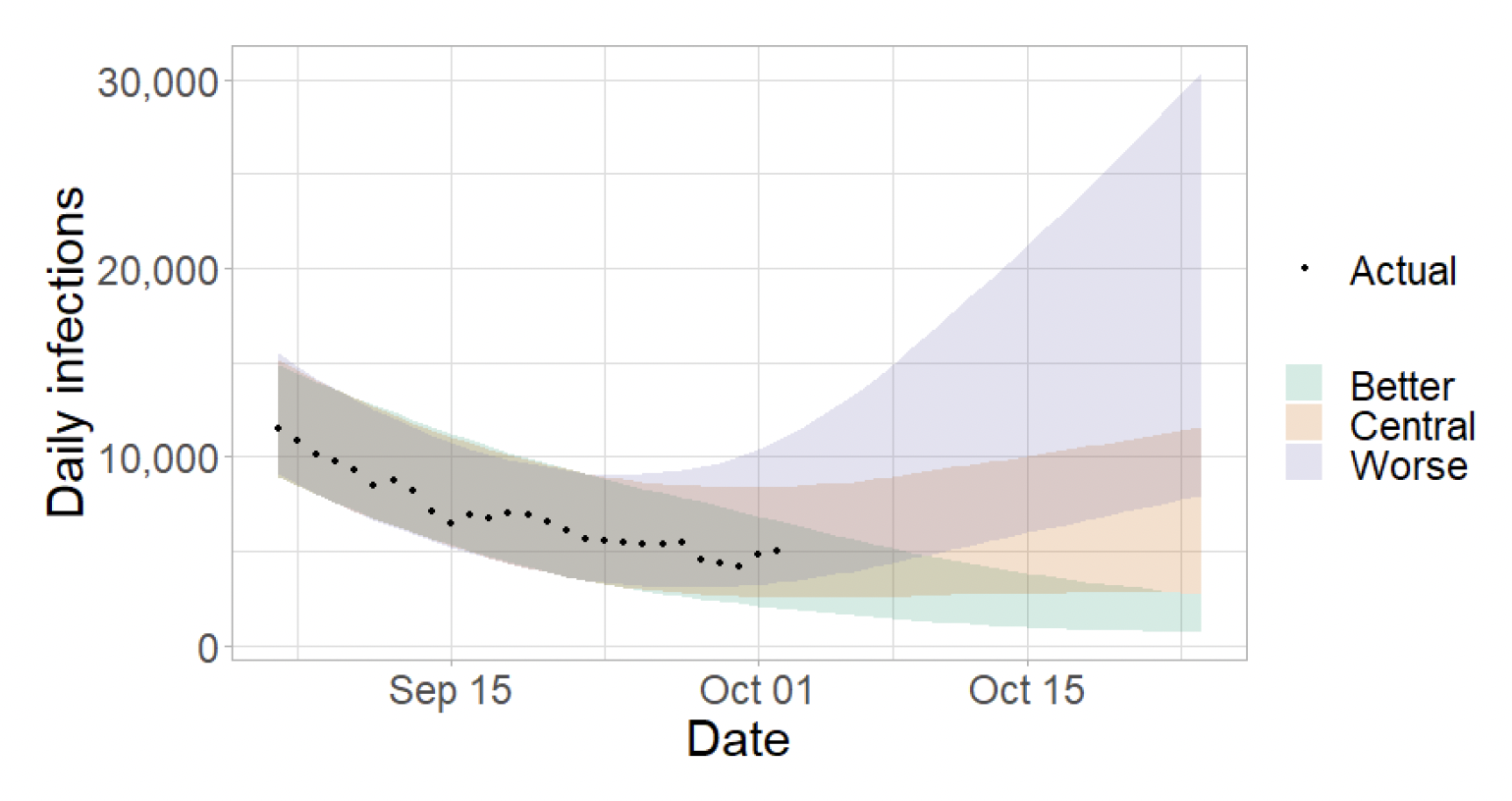
Figure 5 shows the impact of the projections on the number of people in hospital. The modelling includes all hospital stays, whereas the actuals only include stays up to 28 days duration that are linked to Covid-19.
There continues to be uncertainty over hospital occupancy and intensive care in the next three weeks.

Figure 6 shows the impact of the projection on ICU bed demand.

A comparison of the actual data against historical projections is included in the Technical Annex.
What the modelling tells us about projections of hospitalisations and deaths in the medium term
SPI-M produces projections of the epidemic[10] (Figures 7), combining estimates from several independent models (including the Scottish Government's logistics modelling, as shown in Figures 4-6). These projections are not forecasts or predictions. They represent a scenario in which the trajectory of the epidemic continues to follow the trends that were seen in the data up to 4th October and do not include the effects of any future policy or behavioural changes.
Due to an insufficient number of models being submitted this week it has not been possible to produce a reliable set of combined projections of deaths. SPI-M's view is that at least three sets of projections are required to produce a consensus view of the future of the epidemic. It hopes to produce a new set of consensus projections next week.
The delay between infection, developing symptoms, the need for hospital care, and death means they cannot fully reflect the impact of behaviour changes in the two to three weeks prior to 4th October. Projecting forwards is difficult when the numbers of admissions and deaths fall to very low levels, which can result in wider credible intervals reflecting greater uncertainty. The interquartile range can be used, with judgement, as the projection from which estimates may be derived until the 26th October, albeit at lower confidence than the 90% credible interval.
These projections include the potential impact of vaccinations over the next few weeks. Modelling groups have used their expert judgement and evidence from Public Health England, Scottish Universities & Public Health Scotland, and other published efficacy studies when making assumptions about vaccine effectiveness.

What we know about which local authorities are likely to experience high levels of Covid-19 in two weeks' time
We continue to use modelling based on Covid-19 cases and deaths using data to 4th October from several academic groups to give us an indication of whether a local authority is likely to experience high levels of Covid-19 in the future. This has been compiled via UKHSA into a consensus. In this an area is defined as a hotspot if the two week prediction of cases (positive tests) per 100K population is predicted to exceed a threshold, e.g. 500 cases.
The very high peak and subsequent sharp fall in cases in the cities of Edinburgh and Glasgow have resulted in very uncertain model combinations this week. It is therefore likely that the uncertainty is overestimated in these areas and case numbers are in the lower range of the estimate.
Modelled rates of positive tests per 100K using data to 4th October (Figure 8) indicate that, for the week commencing 17th October 2021, there are 29 local authorities which are expected to exceed 50 cases per 100k with at least 75% probability[11].
There are no local authorities which are expected to exceed 300 cases per 100k with at least 75% probability[12].

What can analysis of wastewater samples tell us about local outbreaks of Covid-19 infection?
Levels of Covid-19 RNA in wastewater collected at a number of sites around Scotland are adjusted for population and local changes in intake flow rate and compared to 7 day average daily new case rates derived from Local Authority and Neighbourhood (Intermediate Zone) level aggregate data. See Technical Annex in Issue 34 of these Research Findings for the methodology.
Nationwide, the fall in levels of wastewater (WW) Covid-19 following the September peak appeared to halt this week. In the seven days ending on 4th October, the national average WW levels was around 88 million gene copies per person per day (Mgc/p/d), compared to 97 Mgc/p/d last week (21/9/21 to 27/9/21), with significant variability in levels from observation to observation. In contrast, case rates continue to decline, though both WW and cases are comparable with the July 2021 peak.
Figure 9 shows the national running average trend for the full set of sampled sites, with a small number of unrealistically large outliers excluded. The number of wastewater samples analysed is at a similarly reduced level as the previous week, standing at around 100 samples per week. This means caution is required in interpreting levels at some of the smaller sites or less densely populated local authorities.

What estimates do we have of the number of people experiencing long Covid symptoms?
The Scottish Government is modelling the number of people likely to experience long Covid symptoms. This gives a projection of estimated self-reported long Covid rates in the future, based on Scottish Government medium term projection modelling, as set out in Figure 10.
This modelling estimates that at 24th October 2021 between 56,000 (1.0% of the population) and 124,000 (2.3%) people are projected to experience symptoms for 12 weeks or more after their first suspected Covid infection in Scotland.
These are preliminary results, further data on rates of long Covid and associated syndromes as research emerges are required.

What next?
The modelled estimates of the numbers of new cases and infectious people will continue to be provided as measures of the epidemic as a whole, along with measures of the current point in the epidemic such as Rt and the growth rate. Further information can be found at https://www.gov.scot/coronavirus-covid-19.
We may report on exceedance in future weeks when the background levels of Covid-19 reduces so that it can be useful in identifying outbreaks.
Contact
There is a problem
Thanks for your feedback