National guidance for child protection 2021: consultation report
This report shows the results of the public consultation on the revised national guidance for child protection in Scotland, and our response to the results.
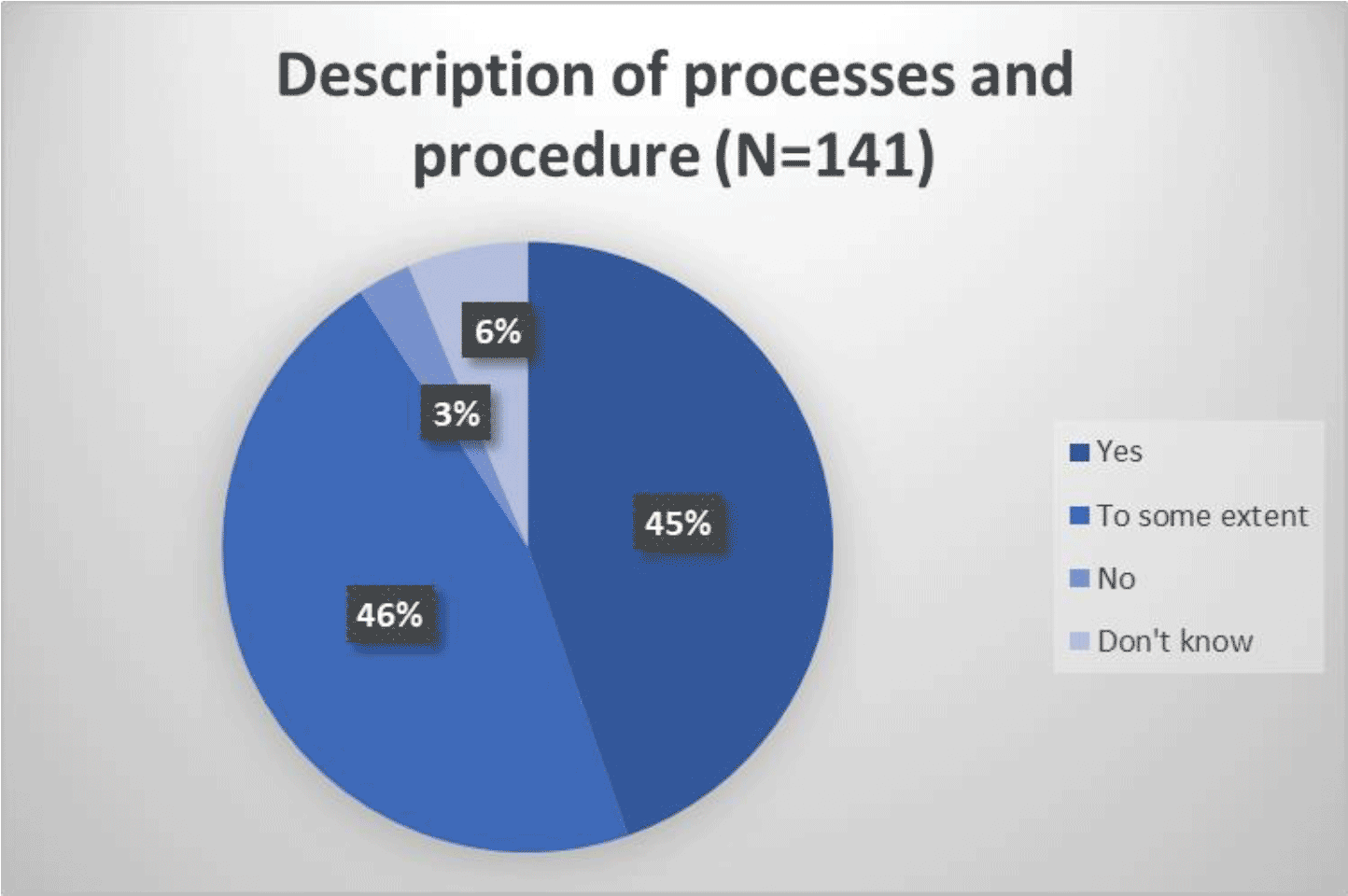
Description of child protection processes and procedure
Q6: Description of child protection processes and procedure - This National Guidance covers the consideration, assessment, planning and actions that are required, when there are concerns that a child may be at risk of harm. It also provides direction where child protection procedures are initiated. This is when Police, Social Work or Health determine that a child may have been abused or may be at risk of significant harm and an Inter-agency Referral Discussion (IRD) will take place.
Are the processes and procedures that lead to and follow IRD clearly described within the Guidance?
Stakeholder Event Themes
The main themes raised at the stakeholder events were:
There was discussion about the age classification of a child and how the guidance should approach this in relation to IRDs.
Whether the intention is to have a national model for IRD?
It would be helpful to have more guidance on the 'pre-IRD' stages and notification of concern.
The named person references are confusing.
Third sector colleagues are currently excluded from IRDs but work closely with families.
Education services should be given a higher profile in the IRD process.
Cross-boundary issues can arise where local authorities have different processes. Cross-border transfers can be complex due to the differences in Scottish and English legislation.
Respondents were relatively evenly divided between those who thought the processes and procedures that lead to and follow IRD are clearly described and those who thought this has been done to some extent (45% and 46% respectively).
Around 95 respondents made a further comment at Question 6.
The consensus was that the section is well-written and clear, and that the detailed description of processes is helpful. However, the resource implications of implementing the revised guidance were noted, and there was a query as to whether additional resources will be made available.
There was a concern that IRD, and JII processes, are very prescriptive and that this may be challenging for some areas. A connected suggestion was that local variations should be acknowledged through the inclusion of a statement that Child Protection Committees, and their constituent members, will be accountable for the adoption (or not) of the processes.
The importance of relationships between practitioners and families, along with person centred risk management that keeps children safe and promotes their wellbeing, was highlighted; it was suggested that this could be more clearly acknowledged within the guidance. It was also suggested that there could be greater emphasis on a strengths-based approach, as the biggest influence on the protection of children.
Other sectors or participants
There were a number of comments about other sectors that should be covered, or given greater coverage, in relation to child protection processes or procedures. These included:
- Education: as referenced elsewhere, education, including early years, should be included as a core agency.
- Health: the role of health professionals in the IRD process could be strengthened. It was reported that health is already seen as a key partner in some local areas, with this including having processes in place to enable health colleagues to initiate an IRD.
- Third Sector: the guidance should emphasise the importance of third sector involvement in the planning and assessment stages for IRDs, not just at the stage of implementation. Third sector involvement in CPPMs should also be strengthened; third sector service providers are often not invited to these meetings, even when they are commissioned to provide services to improve children's wellbeing.
Other observations sometimes related specifically to who should be involved in an IRD and included that:
- A more explicit and comprehensive identification of potential key IRD participants would be beneficial, including third sector agencies, as appropriate.
- Child and Adolescent Mental Health Services (CAMHS) representation at IRD could be helpful where they have current involvement with a child.
- Local young carers services are a point of contact where children are carers.
- It would be helpful if the guidance was more explicit about who can raise an IRD for an unborn child, whether it is the midwife or a family nurse or the paediatrics team?
CPPM
Comments about CPPMs often raised queries, including that:
- Clarity on when cases may progress to a CPPM without an IRD would be welcome, including for example if a family is already being supported.
- It would be helpful to set out when a CPPM may not be appropriate. The guidance appears to suggest that all investigations will lead to a CPPM unless an IRD indicates otherwise.
- Further explanation is required on the relationship between the IRD, any investigation, and the CPPM, including more detail on the role of the Social Worker and the team around the child.
It was noted that the increase from 21 to 28 days for an investigation prior to a CPPM may create additional pressure for families and children, as the overall timescale is potentially lengthened.
Finally, it was suggested that interim safety plans prior to a CPPM should be referred to more consistently in the text (and included in any related flowcharts).
IRD-related comments or suggestions
It was suggested that consideration be given to how the guidance, and new models such as the Scottish Child Interview Model, will be implemented in rural and remote areas as they have different contexts, and operating capacities, from urban settings.
Quality assurance and training related comments included:
- Quality assurance measures should be in place for IRDs and JIIs, including self-evaluation and auditing of IRD cases. Those cases that do not go to IRD should also be evaluated
- There should be guidance on training and supervision for staff participating in IRD processes, including around core competencies.
Approach and process-related comments included:
- The guidance on IRDs should define significant harm and also harm, as the terms appear to be used interchangeably.
- The section on JIIs should be written to take account of the new model of Scottish Child Interview Model.
- Cases of non-familial abuse can be a grey area of practice and require additional guidance, as there is a concern that IRD may be less likely for these cases.
- The IRD process could be clearer in relation to medical examination - some agencies delay further action until a medical has been completed. Specific guidance on mental health examinations was requested, to ensure comprehensive care for children.
- Advice on carrying out debrief sessions after IRDs would be useful in helping staff take account of the impact on wellbeing of themselves and other staff.
16-17-year-olds
It was suggested that further guidance is needed on child protection processes for 16-17 year olds, including in relation to information sharing arrangements. Other comments included that:
- There should be national agreement on the principles for IRDs and JIIs specifically for 16-17 year olds, including a framework for interviews. It was reported that IRDs for this group are more likely to be held later in the day and/or at weekends.
- There is a lack of detail on whether parents or carers should be invited to CPPMs. It is also unclear whether any information a young person provided can be shared with parents or carers if the young person does not give consent.
- Housing staff should be included in IRD guidance in relation to 16-17 year olds, as they are often supporting this vulnerable group.
- In some circumstances, the involvement of an Adult Protection practitioner may beneficial. However, the IRD guidance does not fit into Adult Support and Protection (ASP) statutory processes, and does not support the transfer to ASP, if appropriate.
Contact
Email: Child_Protection@gov.scot
There is a problem
Thanks for your feedback