Quality prescribing for respiratory illness 2024 to 2027 - draft guidance: consultation
We are consulting on this draft guide which aims to optimise treatment outcomes in the management of respiratory illness. Produced by Scottish Government, NHS Scotland and Experts by Experience, it builds on the 2018 to 2021 strategy. It promotes person-centred care, the 7-Steps process for medicine reviews and shared decision-making.
5. Asthma
Asthma
Over five million people are receiving asthmatreatment in the UK. Asthma accounts for 2-3% of primary care consultations, 60,000 hospital admissions, and 200,000 bed days per year in the UK.11
Summary of recommendations in asthma
In all individuals with asthma
- recommend that a patient prescribed six or more inhalers annually is a trigger for timely, priority review - an immediate prescription may be necessary but review should take place before authorisation of the next prescription
- review patients on SABA inhalers alone, clarifying the diagnosis and establishing reasons for SABA only use
- review patients with asthma prescribed SABA and LABA without ICS
- review patients with asthma who have been prescribed an ICS inhaler and do not currently order on their repeat prescription - assess adherence and understanding of treatment to establish appropriate use of SABA inhalers
- review inappropriate use of high strength corticosteroid inhalers (maintaining patients at the lowest possible dose of inhaled corticosteroid)
- reductions in high dose ICS should be considered every three months, decreasing the dose by approximately 25–50% each time, arranging regular review as treatment is reduced
- issue a steroid treatment card to patients on inhaled high dose corticosteroids - steroid emergency card may also be required
- review montelukast at four to eight weeks following initiation to ensure a response and that therapy is still required
In severe asthma
- identify patients with severe asthma and where modifiable risk factors are addressed and asthma care remains suboptimal, refer to secondary care for treatment optimisation
In children with asthma
Whilst this guidance is not for children and prescribers should refer to guidance on asthma management in children, there are two medication safety points to highlight:
- record regular growth monitoring when treating children with ICS
- ensure children on medium / high-dose ICS are under the care of a specialist paediatrician
Principles of prescribing for asthma
Asthma is a chronic respiratory condition associated with airways inflammation and hyper-responsiveness.
The aim of treatment is control of the disease with:
- no daytime symptoms
- no night-time waking due to asthma
- no need for rescue medication
- no asthma attacks
- no limitations on activity including exercise
- minimal side effects from medication
Inhaled therapy is used as the main treatment of asthma, which should be started at the level most appropriate to the initial severity of asthma symptoms. The aim is to achieve and maintain early control by increasing treatment as necessary and decreasing unnecessary treatment when control is good. 12 Personalised asthma action plans, agreed with the health care professional, empower individuals to gain control using the minimum dosage of inhaled corticosteroid. 12
Inhaled corticosteroids are the most effective preventer drug to achieve treatment goals. Add-on therapy, including long-acting beta agonists (LABA), leukotriene antagonists, long-acting muscarinic antagonist (LAMA) and theophyllines, should only be initiated after checks on inhaler technique, adherence and elimination of trigger factors. People with asthma should be reviewed at least annually to determine whether their existing treatment regime is adequately managing their symptoms.
Inhaler device selection is important. People with asthma should receive training on how to use their inhaler device and be able to use it. 12 The environmental impact of inhalers is a key consideration and prescribers are asked to consider inhalers with a lower global warming potential where appropriate for the individual (see chapter 10).
To prescribe most effectively for people with asthma, we recommend the ‘what matters to you?’ principles and the Polypharmacy 7-Steps approach. Table 1 outlines the main principle for treating patients with asthma.
Table 1: Principles of treating patients with asthma
Polypharmacy review 7-Steps
1 What matters to the patient? Ask the patient what matters to them?
- How does the condition affect patients' day to day life/activities?
- Take account of co-morbidities when prescribing for asthma, by using the Polypharmacy 7-Steps approach
- Do environmental prescribing issues matter? (see chapter 10)
2 Identify essential drug therapy Asthma diagnosis confirmed?
- Fractional exhaled nitric oxide (FeNO) test could be used as an optional investigation to test for eosinophilic inflammation when there is diagnostic uncertainty 12
- Ensure asthma therapy is optimised as per local / SIGN / BTS guidelines 12
- Assess adherence, review inhaler technique and eliminate trigger factors prior to initiating or adjusting therapy
- Confirm ongoing need for and effectiveness of medication and screen for side effects
3 Does the patient take unnecessary drug therapy? Assess adherence and ensure patient understands treatment regime, using an asthma action plan.
- Discuss SABA use with patients prescribed more than three SABAs annually as this is a marker of poor control
- Consider the use of Maintenance and Reliever therapy (MART) regimen in patients where there is poor control or adherence when on separate medium dose ICS, LABA and SABA 12
- When asthma is controlled and stable, clinicians should consider stepping down inhaled corticosteroid (ICS) treatment, slowly, every three months reducing by 25-50% each time, monitoring for deterioration 12
4 Are therapeutic objectives being achieved? Can the patient use their inhalers properly?
- Any patient who has asthma medicine started or changed should be reviewed within three months
- Medication should be titrated to a dose which balances maximum clinical efficacy with minimal risk and stopped if found to be ineffective or if adverse effects outweigh benefits
- If asthma is not adequately controlled on recommended initial or additional therapies, as per BTS/ SIGN 12, patient should be referred for specialist assessment
- Exacerbations should be considered as an opportunity to review therapy, optimise treatment and ensure self-management plans are updated
- Once the dose is stable and effectiveness has been established, ongoing review should occur as clinically appropriate, with follow up at least annually if asthma control has been achieved
- For environmental considerations, consider switch to DPI inhalers for patients with asthma who:
- have an adequate inspiratory flow (e.g., use an In-Check device)
- have been stable for two years
- have had no asthma attack for two years
- have never been admitted to hospital /ITU
- are not under secondary care review
- If there is any concern that an individual is at higher risk of asthma attack, or risk of severe attack, then remain on a pMDI reliever plus a spacer device 12 (see advice in table 14, SIGN 158)
- Consider switch to pMDI with lower global-warming potential where this is clinically appropriate (e.g. Salamol®, Airomir®)
- Ensure awareness of how allergies (pet, pollen, dust), air pollution can affect respiratory conditions
- Vaccinations should be offered if not up to date as per national guidance
- Individuals should be encouraged to engage in appropriate physical activity - social prescribing such as exercise would be dependent on ability
- A breathing exercise program can reduce symptoms
- Smoking cessation should be advised and the adverse effects of smoking on children highlighted. Offer appropriate support - signpost patients to the NHS inform Quit Your Way Scotland website (includes community pharmacy services)
- Weight reduction should be considered in patients who are overweight (BMI 25 – 29.9) or obese (BMI >30) to reduce respiratory symptoms 12
5 Is the patient at risk of Adverse Drug Reactions (ADR)s or suffer actual ADRs?
- Consider risk factors for future risk of asthma attack and address these when prescribing - for instance, patients:
- with an asthma attack in the past
- who have received more than one course of oral corticosteroids in one year
- who have received more than six SABA inhalers a year should be prioritised for an asthma review
- on high dose inhaled steroids
- with multiple morbidities e.g. COPD, depression, Gastro-oesophageal reflux disease
- with poor asthma control
- who smoke
- Steroid treatment cards should be provided to patients on high dose steroids (both oral and inhaled). A steroid emergency card may also be required. A national review will establish how to identify patients utilising Scottish Therapeutics Utility (STU) following the Health Improvement Scotland (HIS) guidance Steroid Emergency Card 13
- Review risk of osteoporosis if on long term or frequent (more than three or four courses a year) oral corticosteroid treatment 14
- Take measures to reduce the risk of and increase awareness of oral thrush - ensure correct technique to reduce incidence - a spacer device is recommended for use with a pMDI and will reduce oral thrush side effects
- Yellow card reporting of true ADRs
6 Sustainability
- Opportunities for sustainable prescribing and cost minimisation should be explored but only considered if effectiveness, safety or adherence would not be comprised
- For new drugs, ensure prescribing is in line with Health Board formulary recommendations
7 Is the patient willing and able to take drug therapy as intended?
A personalised asthma action plan is key to this approach, with focus on inhaler technique, peak flow monitoring, worsening symptom advice, appropriate use of a spacer and avoidance of new trigger factors
- Make patient aware of support information e.g. the My Lungs My Life website (appendix 1)
- Non-attenders should be followed up – alternative strategies to encourage engagement may be required (e.g. through community pharmacy / Near Me / telehealth acknowledging limitations)
- Agree with the patient arrangements for repeat prescribing - signpost to Medicines Care and Review service in Community Pharmacy where appropriate
Prescribing issues to address
The issues identified are priority areas of prescribing, where there is unwarranted variation within Health Boards and where accurate prescribing data can be provided. Ensuring asthma medicines are reviewed and optimised will reduce this unwarranted variation. The indicators focus on ensuring quality prescribing and any of the recommendations made follow national clinical guidance. 12 The indicators included are as follows:
- prescribing of short-acting beta-agonists (SABA) per annum
- prescribing of inhaled high dose corticosteroids
- prescribing of long-acting beta-agonists (LABA) without inhaled corticosteroids (ICS)
- prescribing of SABA only
- prescribing of Leukotriene receptor antagonists
Prescribing of short-acting beta-agonists (SABA)
Evidence for review of SABA
It is essential that patients who appear to be overusing SABA inhalers are assessed for control of symptoms. Asthma control test (ACT) questions15 highlight that a patient is not controlled if they use a SABA inhaler three or more times in a week.12 The National Review of Asthma Deaths (NRAD) report16 found that patients who used more than 12 inhalers per year were at a greater risk of uncontrolled asthma and sudden death. There was evidence of under-prescribing of preventer medication. Use of 12 SABAs in one year implies the use of 46 puffs in one week and for six SABAs a year is 23 puffs a week.17 In the SABINA study,18 an association across all asthma severities was found between high SABA use, of more than three inhalers per year, and an increase in exacerbation rates and healthcare utilisation. 19 It is crucial that patients understand the importance of when and how to use their inhalers and of adherence to therapy with their preventer inhaler.17
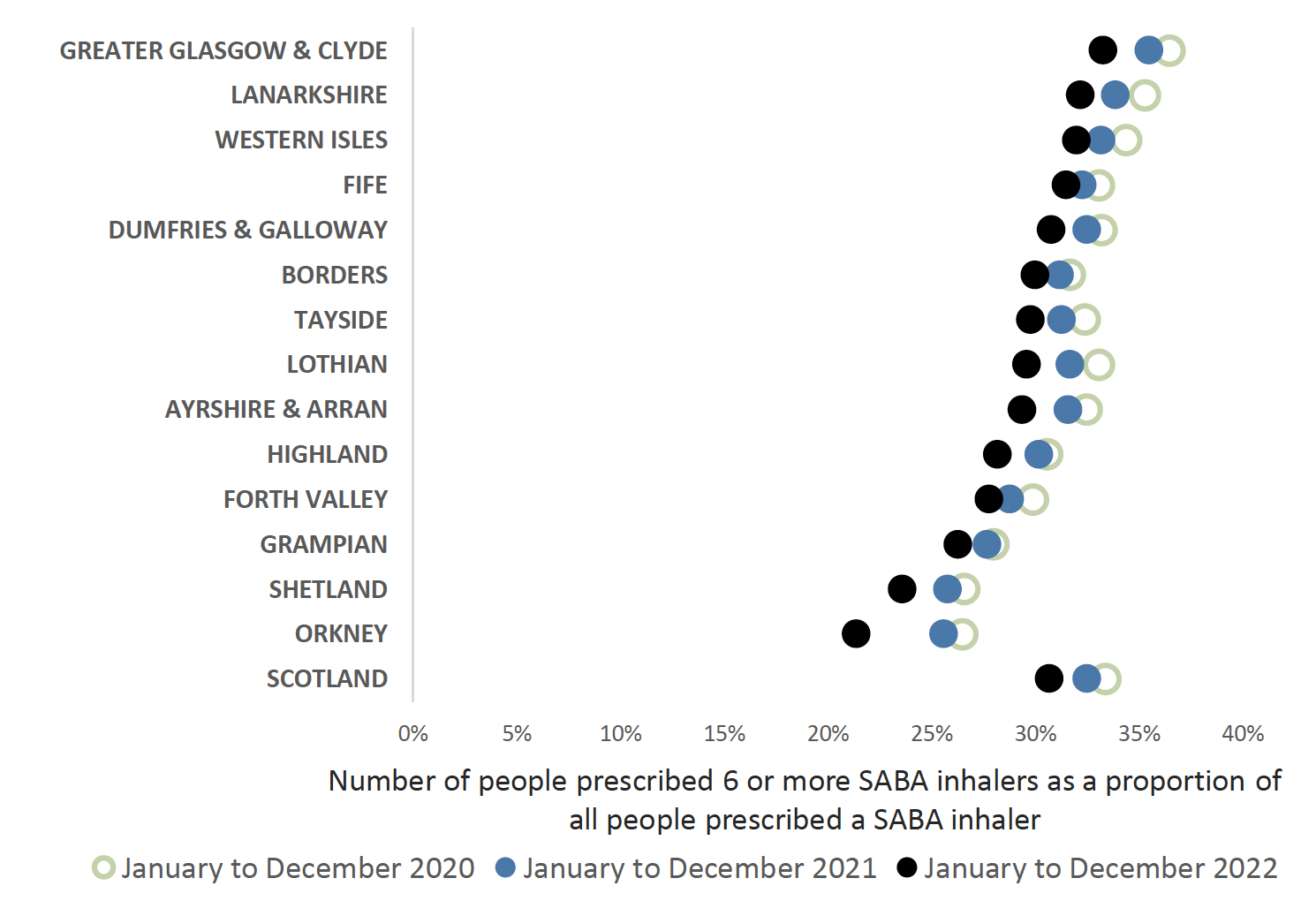
The main focus of an asthma review is to ensure that the individuals' condition is well controlled, they are prescribed the optimum inhaler therapy in alignment with current guidance and are using their inhalers effectively. We know that there are many people with asthma in Scotland who are prescribed six or more SABA inhalers in 12 months (see chart 1 below). This is associated with a higher rate of exacerbations and hospitalisation.18
Following clinical consensus regarding asthma control, this indicator has been reduced from the previous 12 SABA inhalers prescribed annually to recommend that a patient prescribed six or more inhalers annually is a trigger for timely, priority review (see chart 1). This should ideally take place before the issue of the next prescription.
The guide includes a chart of people prescribed three or more SABA inhalers as an aspirational level, as a person with well-controlled asthma would need no more than this (see chart 2). This should be discussed at the annual routine review. This indicator is a guide and is unable to distinguish between people with Asthma and COPD.
It should be noted that emergency supplies of SABA inhalers are possible to obtain from the community pharmacy. Liaison with community pharmacy colleagues is advised to help reach those people with asthma who may be poorly controlled and do not attend asthma reviews.
The Scottish Therapeutic Utility (STU) software (chapter 12) is recommended, to support GP Practices to identify individuals with asthma who are over-reliant on SABA inhalers using practice coding.

Charts one and two highlight that the number of SABA inhalers that patients have received annually has remained fairly constant, after a slight increase during April 2020 – March 2021 across NHS Scotland. This may be due to prescribing of SABA inhalers in response to the COVID-19 pandemic.
Prescribing of inhalers with dose counters may assist in monitoring adherence with inhalers and to ensure that individuals know how many doses remain in the inhalers to prevent medicine waste. 20
Review of high SABA pMDI use
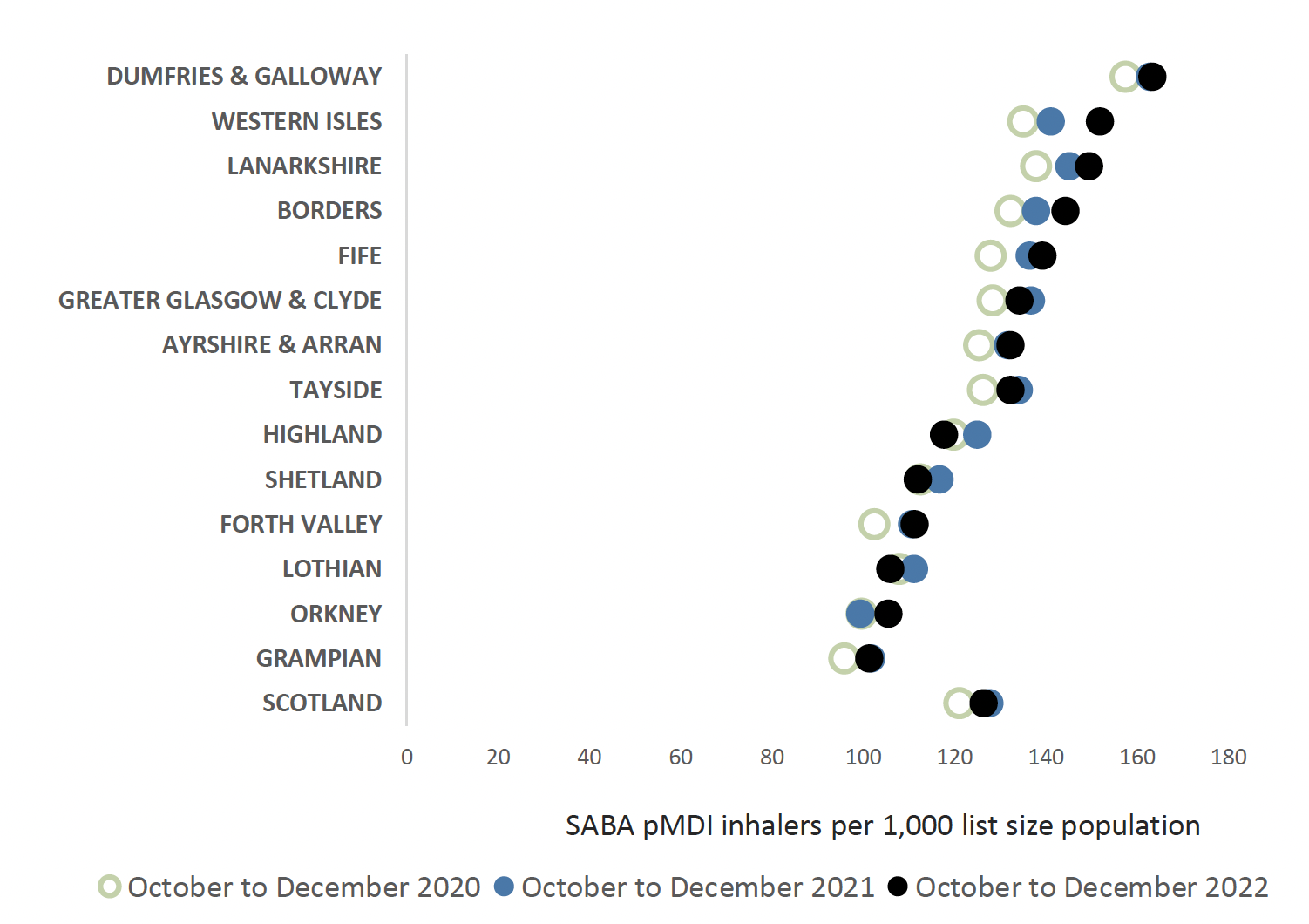
A recent study found that SABA inhalers accounted for the majority of pMDIs prescribed and advocated better disease control to reduce SABA inhaler use and therefore CO2 emissions 21 (see environmental chapter). Approximately 70% of all inhalers in NHS Scotland are prescribed as an pMDI. The UK has a high proportion of pMDI use (70%) compared with the rest of Europe (< 50%) and Scandinavia (10–30%). Figures from Scandinavia show a lower rate of deaths. 22
Reviewing patients regularly and providing education on good control of respiratory disease and optimising treatments will reduce SABA inhaler use, improving patient care and disease control. This will also support reduction in CO2 emissions, which is a target for NHS Scotland (see environmental chapter). Chart 3 below highlights the proportion of SABA pMDI inhalers alone prescribed in each NHS Board.
Prescribing of high dose corticosteroid inhalers
There are safety concerns regarding the inappropriate use of high strength corticosteroid inhalers and the importance of ensuring that the patient’s steroid load is kept to the minimum level whilst effectively treating symptoms. It is recognised that some patients will require treatment with high-dose ICS. This indicator acts as a guide for highlighting use of inhaled high dose corticosteroids but is unable to distinguish between patients with asthma and COPD. The STU software will allow GP practices to identify patients within each cohort for review.
Patients on inhaled high dose corticosteroids (or multiple steroid preparations) should be issued with a steroid treatment card (blue), see figure 4. There is an additional steroid emergency card (figure 5) which alerts patients who are dependent on long term steroids and at risk of adrenal insufficiency to the potentially serious, systemic side effects from them. A full list of steroid doses to assist with determining who should be issued with a steroid emergency card (red) is contained within the Healthcare Improvement Scotland advice 13 and STU software will assist identification of these patients. The most concerning side effect is adrenal suppression, others include growth failure; reduced bone density; cataracts and glaucoma; anxiety and depression; and diabetes mellitus. 23

Chart 4 shows that high dose corticosteroid inhaler prescribing has increased in most NHS boards since 2020.

Whilst this guidance is not for children and prescribers should refer to guidance on asthma management in children, there are two of medication safety points to highlight. Prescribing of high dose inhaled corticosteroids in children, aged under 12 years, is of particular concern due to long term safety concerns. Children on high dose corticosteroids should be reviewed and under the care of paediatricians with a special interest in respiratory medicine. Transition from child to adult services should be considered for children with unstable asthma or co-existing risks, such as food allergies and reviews carried out to facilitate this. There is a report available using the STU utility to identify high dose corticosteroid use in children under 12 years.
When treating children with ICS 12 :
- it is important to record growth (Height and weight centile) on an annual basis using the same equipment 12 (unreliable indicator of adrenal suppression) - if there are concerns regarding growth, advice should be sought from a paediatrician
- high-dose ICS should be used only under the care of a specialist paediatrician
- adrenal insufficiency should be considered in any child with shock and/or reduced consciousness who is maintained on ICS
Evidence for review of high dose inhaled corticosteroids
SIGN 158 recommends the following for adults and children.
Patients should be maintained at the lowest possible dose of inhaled corticosteroid. Reduction in inhaled corticosteroid dose should be slow as patients deteriorate at different rates. Reductions should be considered every three months, decreasing the dose by approximately 25–50% each time.
It is important to arrange for a regular review of patients as treatment is reduced. When deciding the rate of reduction, it is important to take into account the following aspects: the severity of asthma, the side effects of the treatment, time on current dose, the beneficial effect achieved, and patient preference.
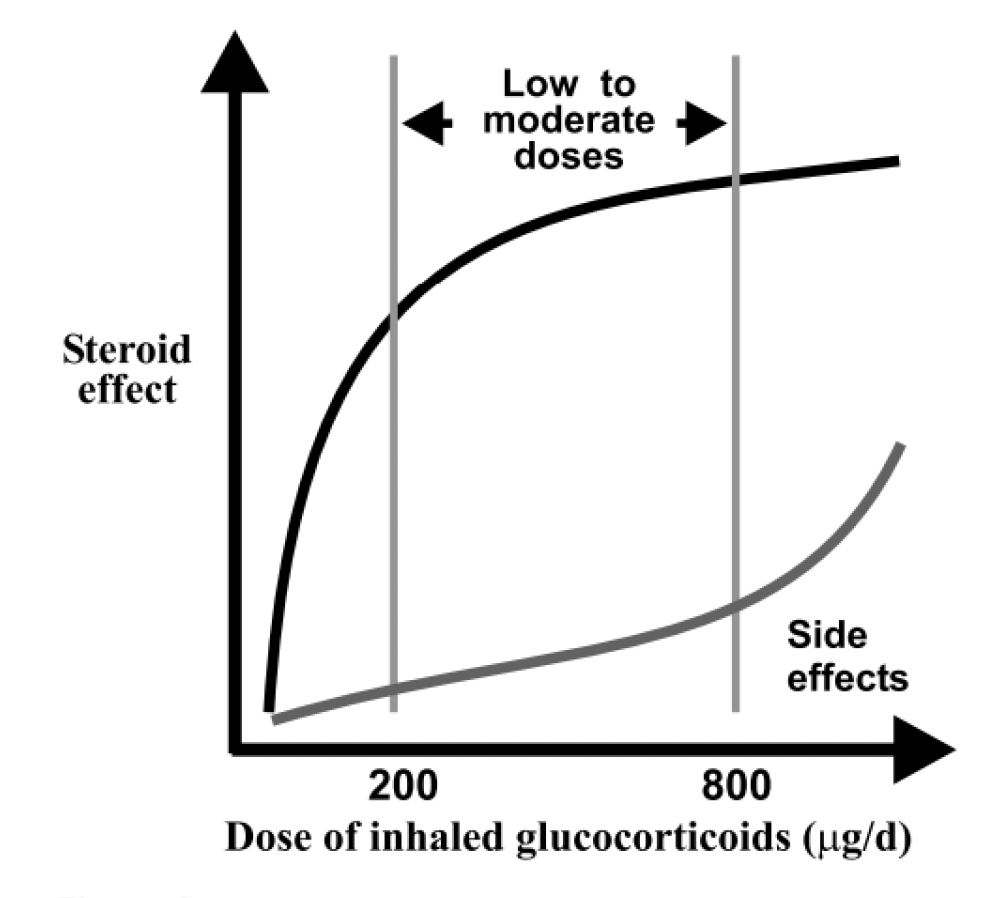
The dose – response curve for inhaled corticosteroids (figure 6) 24 shows the difference in clinical effect and side effects when a corticosteroid dose is increased. At doses of 800 micrograms per day and above, the clinical benefit of increasing inhaled corticosteroid dose is outweighed by increase in side effects.
Number of Inhaled corticosteroids prescribed per annum
People who have been prescribed an ICS inhaler and do not order on repeat prescription should be checked for adherence and understanding of preventer treatment and to establish appropriate use of SABA inhalers. The National Review of Asthma Deaths (NRAD) report 16 highlighted that some people at risk of uncontrolled asthma / sudden death had under used preventer medicines. Most ICS inhalers (pMDIs and DPIs) have a dose counter and that may be used to aid understanding of adherence based on an individual’s asthma management plan.
Conversely, some people may over-order inhalers for various reasons, such as poor understanding of therapy. A review would be advised to explore this. Use of the STU software is recommended for GP practices to identify patients receiving 14 or more ICS inhalers a year (see chapter 12).
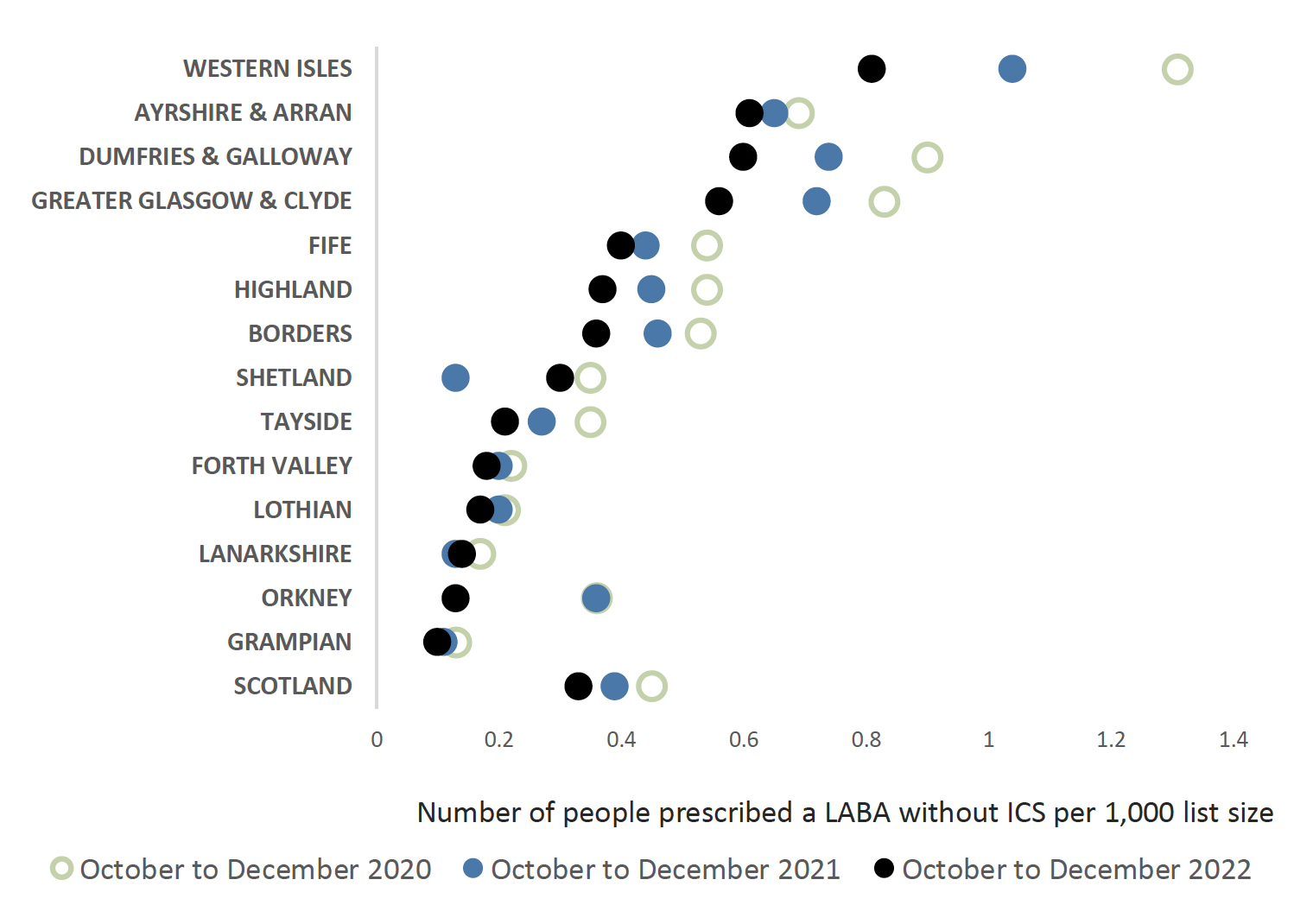
Prescribing of SABA plus LABA without ICS
The NRAD report 16 also highlighted that patients who were at higher risk of death due to asthma had a LABA prescribed without an ICS. As is clear from chart 5 the number of people without an ICS prescribed is small and continues to reduce. Some of these patients may have a COPD diagnosis in which case prescribing of a LABA without an ICS would be reasonable.
Prescribing of SABA only
This indicator highlights the proportion of patients who receive a SABA inhaler in the absence of other inhalers. SIGN 158 states that on diagnosis of asthma, patients be considered for monitored initiation on low dose ICS plus a SABA as required. Patients on SABA inhalers alone should be reviewed, establishing reasons for SABA only use, such as COPD diagnosis, viral wheeze and COVID-19 symptoms.
Using STU software is recommended within GP practices and will allow identification of individuals coded with asthma on a SABA inhaler only (see chapter 12).
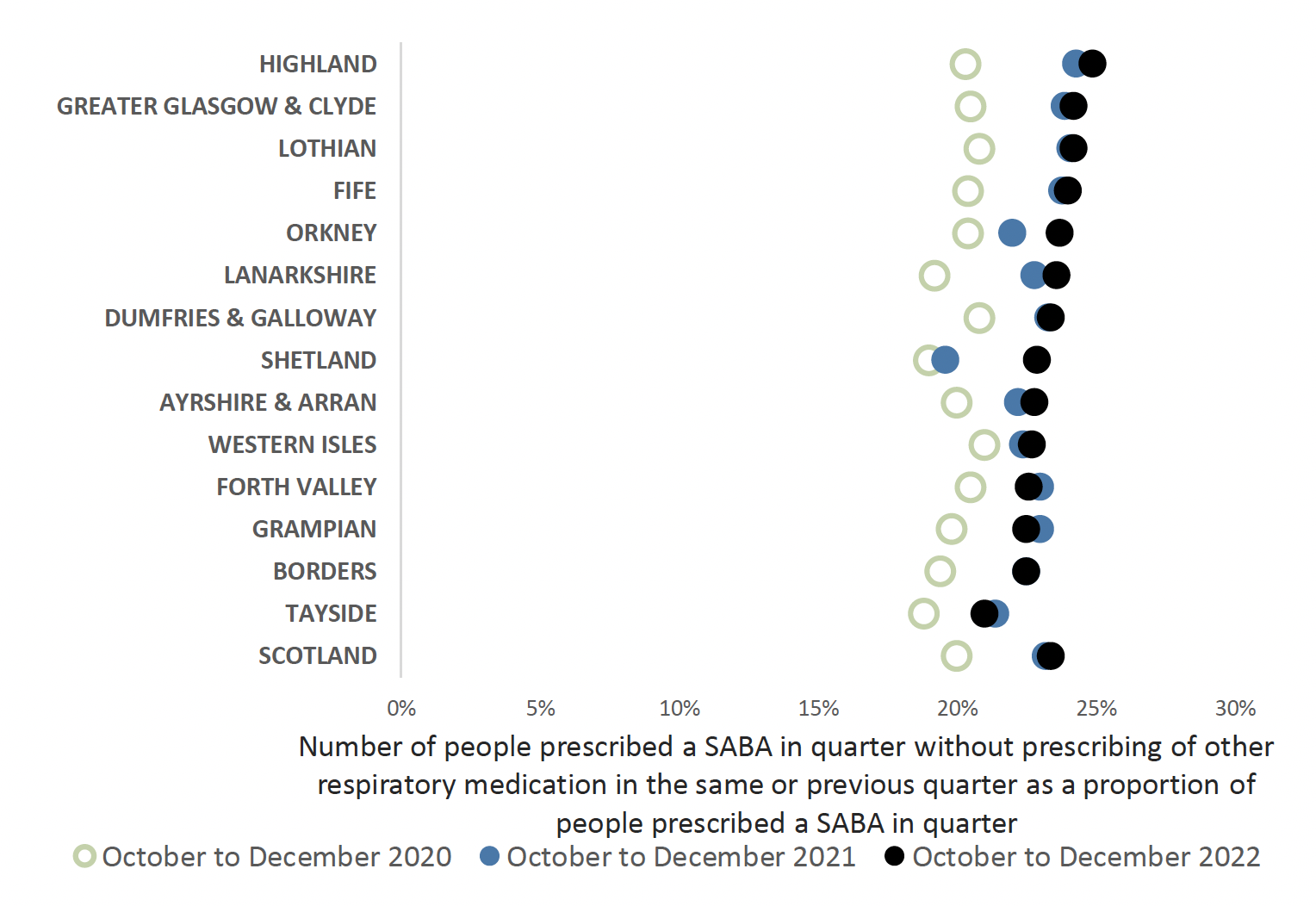
Chart 6 shows that in NHS Scotland approximately 23% of people being prescribed a SABA inhaler are not prescribed other inhaler therapy. As per national asthma and COPD guidelines, very limited numbers of patients should be prescribed SABA inhalers only.
Prescribing of Montelukast (leukotriene receptor antagonist)
Montelukast can be used as an additional add on therapy for asthma in adults. If control remains suboptimal after the addition of an inhaled LABA to low-dose ICS then either:
- increase the dose of inhaled corticosteroids to medium dose
or
- consider adding a leukotriene receptor antagonist 12
Chart 7 below highlights prescribing of Montelukast, which shows a variance in NHS Boards across Scotland. Overall prescribing appears to have increased. Montelukast should be reviewed four to eight weeks following initiation 25 to ensure that there has been a response to therapy and that it is still required.

The Medicines and Healthcare products Regulatory agency (MHRA) issued a reminder regarding the known risks of neuropsychiatric reactions with montelukast.26
A recent EU Review 27 of montelukast confirmed the known risks and that the magnitude was unchanged. The review highlighted that there had been some delays in recognising that neuropsychiatric reactions were a potential side effect to montelukast. Consider the benefits and risks of continuation of prescribing, should these side effects occur.
Severe Asthma
Severe asthma is defined as asthma that is uncontrolled despite adherence to optimised maximal inhaled therapy and management of contributory factors or worsens when high dose treatment is decreased. 28
Poorly controlled and/or unrecognised severe asthma is a significant problem, leading to morbidity and mortality. Severe asthma is associated with poor asthma control, impaired lung function and repeat exposure to oral corticosteroids (OCS) which can lead to further OCS-related adverse effects such as diabetes, adrenal insufficiency, and osteoporosis.
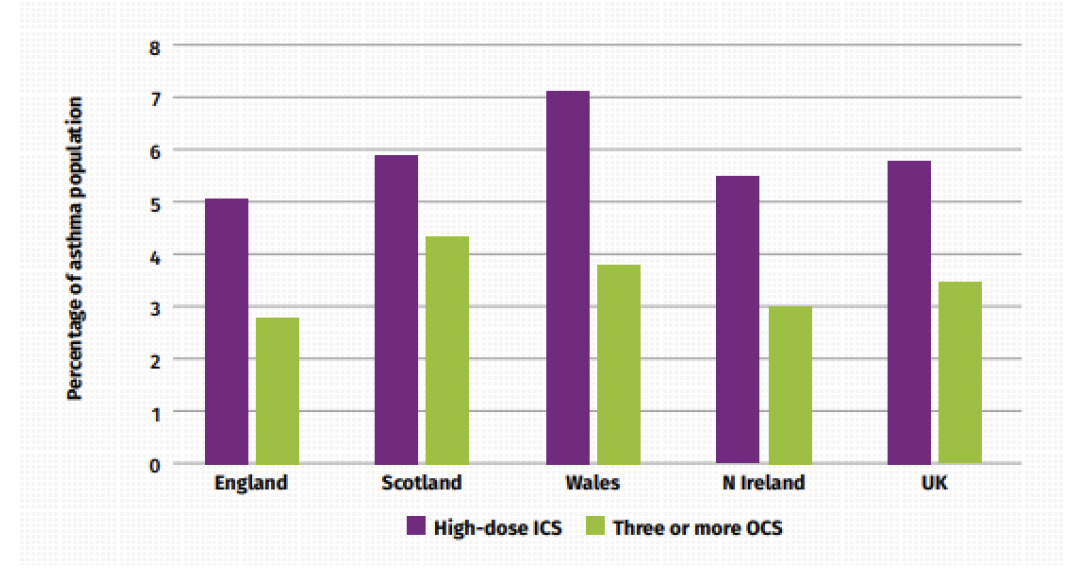
Severe asthma is estimated to affect 3% to 5% of the asthma population. Scotland has higher rates of difficult and severe asthma compared to the rest of the UK. 29
Proxy measures of inhaled high dose corticosteroids (ICS) or number of courses of oral corticosteroids (OCS) treatments as indicators of severe asthma have been suggested. 29 Figure 7 below outlines the differences in difficult or severe asthma prevalence, based on the indicators of high-dose ICS or those receiving three or more OCS courses across the nations in the UK in 2016. 29 For three or more OCS prescriptions, Scotland has the highest figure in the UK, with 4.3%, compared to the UK figure of 3.4% of the asthma population.
Early identification of at-risk patients with asthma is key to ensure prompt referral to specialists for consideration of Monoclonal antibody (mAb) therapy where appropriate. Pathways have been developed to support the identification and management of patients at risk of severe asthma. 30
Criteria to identify patients at risk of severe asthma:
- ≥6 SABA prescriptions in previous 12 months
or
- ≥2 asthma exacerbations / OCS prescriptions in previous 12 months 1–3
or
Modifiable risk factors such as smoking status, inhaler technique, adherence and housing conditions should be addressed and a referral made where asthma control remains suboptimal 30. Scottish Therapeutic Utility (STU) software will aid identification of these patients within GP practices.
Monoclonal antibodies (mAb) are a type of biologic drug that can be used to treat severe asthma. They target specific biological processes to reduce inflammation in the lungs and currently either target ‘allergic’ asthma or ‘eosinophilic’ asthma. There are currently four mAbs approved by the Scottish Medicine Consortium (SMC) for Scotland; omalizumab, mepolizumab, benralizumab and dupilumab. These medications have been shown to significantly reduce asthma exacerbations, hospital admissions and oral corticosteroid use. 31, 32, 33, 34 The SMC has set strict eligibility criteria for patients receiving these drugs to ensure that they are used for patients most likely to benefit and are used in the most cost-effective way. Consequently, mAbs are included in SIGN/BTS and NICE clinical guidance for the treatment of severe asthma. 12, 35
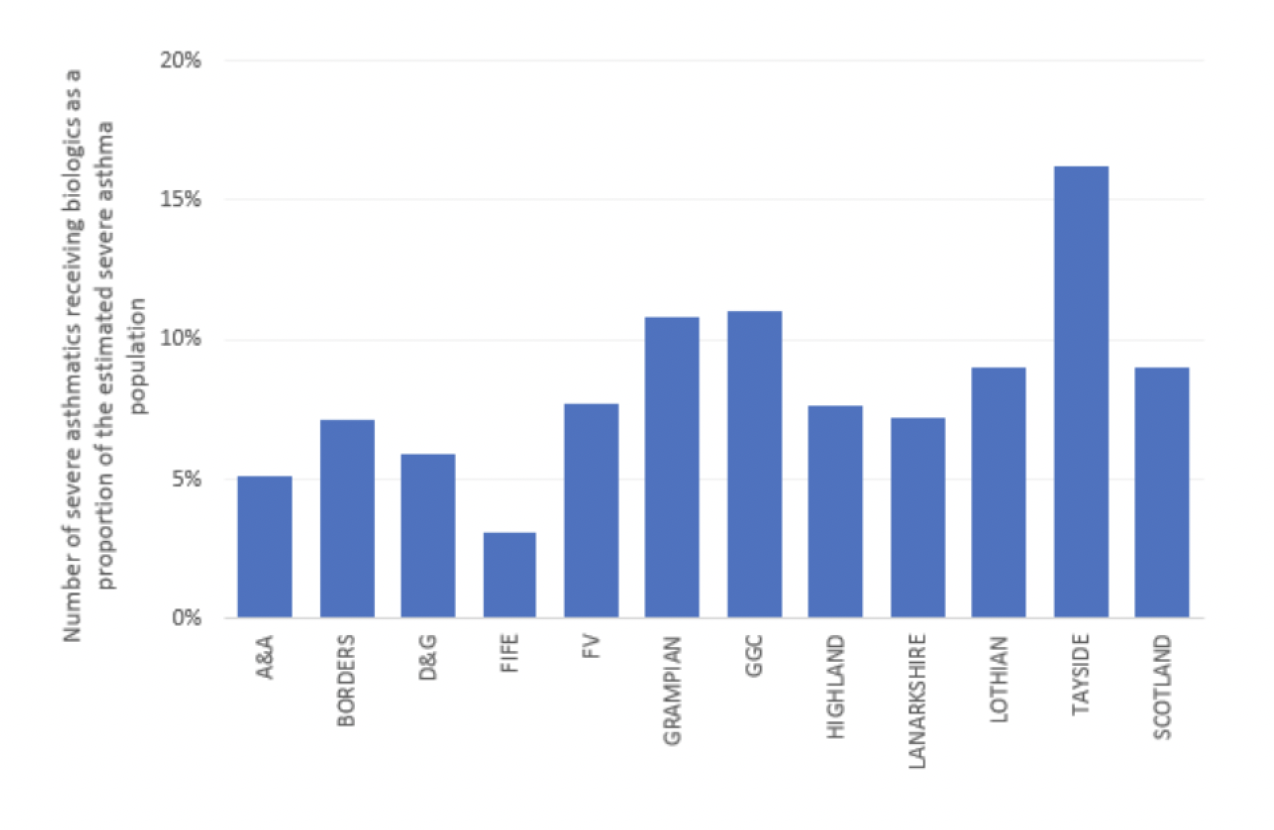
It has been previously estimated that 20% of eligible patients with severe asthma, received treatment with mABs in the UK. 29 The Accelerated Access Collaborative estimated this as 17-21% of eligible patients in England. 36 A benchmarking exercise was completed across NHS Scotland identifying adult patient numbers prescribed mAbs as a proportion of the estimated severe asthma population (shown in chart 8) showing wide variation in prescribing based on weighted population. A prevalence of 6.4% was assumed for asthma, based on the Scottish Public Health Observatory figures, and severe asthma estimated as 4% of this. Uptake and use of mAbs for the management of severe asthma varies across Scotland. Ongoing work is required to increase early identification, referral and assessment of at-risk patients.
Environmental considerations in severe asthma
A report published by the Sustainable Health care coalition 37 estimated that the greenhouse gas (GHG) emissions associated with a person’s management of severe asthma is reduced by approximately 50% through the use of mAb therapy.
This reduction is due to the combined effects of improved symptom control, reduced exacerbations and a decrease in hospital admissions. These trends directly affect the environmental impact associated with asthma management and are important steps towards more sustainable treatment.
Asthma case study
Case summary – Asthma
Background Details - (Age, Sex, Occupation, baseline function)
- 47-year-old female
- Works as cleaner in local high school, but currently off sick
- Has had 16 courses oral prednisolone therapy in 12 months without any face-to-face review with any clinician. Ordered 24 salbutamol pMDIs in 12 months
- Breathless, nocturnal wheeze most nights
- Never tested positive for Covid
History of presentation/ reason for review
Referred to Respiratory Clinical Nurse Specialist due to OCS use and high-volume ordering salbutamol despite current treatment with Airflusal® pMDI 250/25 Two puffs twice daily. Worsening symptoms past year.
Multiple courses of oral prednisolone therapy
Current Medical History and Relevant Co Morbidities
Asthma
Current Medication and drug allergies (include OTC preparation and Herbal remedies)
- Airflusal® pMDI 250/25 two puffs twice daily, only ordered six inhalers in 12 months
- Salbutamol pMDI two puffs, as required, 24 inhalers ordered in 12 months
Lifestyle and Current Function (inc. Frailty score for >65yrs) alcohol/ smoking/ diet/ exercise
Lives with husband and three children. Has two dogs, one cat.
Current smoker, 10 cigarettes per day with 18 pack years
Overweight with BMI 31.
Little motivation to engage with physical activity.
Results e.g. biochemistry, other relevant investigations or monitoring
Asthma Control Test (ACT) 7/25
RadioAllergosorbent Test (RAST) – High positive dogs, moderate positive cats, low positive pollen, dust mite. Await Total IgE and aspergillus serology.
Normal eosinophils. TFTs, FBC, Us and Es, Bone, Glucose, ANA, ANCA, CRP, Iron studies and B12- normal.
Referred Chest X-Ray (CXR) and Pulmonary function tests (PFTs)
Most recent consultations
First consultation: discussed symptoms and did ACT which was 7/25. Carried out full asthma serology screen. Referred for full PFTs, CXR and DEXA scan
Chest exam-NAD. SpO2 98% room air.
Discussed concerns over multiple prednisolone courses, high volume salbutamol use and poor adherence to Airflusal® looking at the prescribing in the context of symptoms and ACT score, discussed adherence to preventer therapy.
Agreed move to Fobumix® Easyhaler® DPI 320 two puffs twice daily and Easyhaler® salbutamol as inhaler technique poor with MDI and good with Easyhaler® and also discussed this in line with health board’s green agenda. Discussed physiology of asthma and concerns as identified at risk.
Explained side effect risks from prednisolone and need for DEXA.
Discussed smoking cessation and Very Brief Advice (VBA) given. Will consider referral to Quit Your Way.
Full asthma screen and review following week.
Follow up appointment:
Given blood results and explained awaiting Total IgE and Aspergillus serology. Discussed addition of Montelukast given RAST positivity and pets. Agreed.
Await date for PFTs and CXR
Further education and discussion around managing asthma.
Aware dependent on full results may refer onto Difficult Asthma Clinic
Personalised Asthma Action Plan discussed and agreed and written copy issued. Advised that this may change dependent on results
Further appointment made for four weeks
1. Aims
What matters to the individual about their condition(s)?
Review diagnoses and identify therapeutic objectives with respect to:
- Identify objectives of drug therapy
- Management of existing health problems.
- Prevention of future health issues
Person specific issues to address
- Worsening symptoms of asthma and poor control, resulting in multiple courses of oral steroids and high volume of salbutamol use
- Getting back to work as a cleaner
2. Need
Identify essential drug therapy
Identify essential drugs (not to be stopped without specialist advice)
- Drugs that have essential replacement functions (e.g. levothyroxine)
- Drugs to prevent rapid symptomatic decline (e.g. drugs for Parkinson’s disease, heart failure)
Person specific issues to address
- Inhaled corticosteroids for asthma control, currently prescribed as a combination MDI, Airflusal® (not being ordered regularly)
3. Need
Does the individual take unnecessary drug therapy?
Identify and review the (continued) need for drugs
- What is medication for?
- with temporary indications
- with higher than usual maintenance doses
- with limited benefit/evidence of its use in general
- with limited benefit in the person under review EPT/Polypharmacy/2022-08-30/Paper">(see Drug efficacy & applicability (NNT) table)
Person specific issues to address
- Salbutamol is used frequently (24 inhalers ordered in 12 months), which would be unnecessary if preventer therapy used effectively
- Past frequent courses of oral steroids (16 courses in 12 months) which increases potential for adverse effects
4. Effectiveness
Are therapeutic objectives being achieved?
Identify the need for adding/intensifying drug therapy in order to achieve therapeutic objectives
- to achieve symptom control
- to achieve biochemical/clinical targets
- to prevent disease progression/exacerbation
- is there a more appropriate medication that would help achieve goals
Person specific issues to address
- Discussion and education regarding adherence to preventer therapy and salbutamol use
- Checked inhaler technique with MDI to ensure able to use
- Inhaler changed to a DPI (Fobumix® Easyhaler®, containing an ICS/LABA) as MDI technique was poor
- RAST positivity and presence of pets at home, therefore addition of montelukast to trial
5. Safety
Does the individual have ADR/ Side effects or is at risk of ADRs/ side effects?
Does the person know what to do if they’re ill?
Identify individual safety risks by checking for
- If the targets set for the individual appropriate?
- drug-disease interactions
- drug-drug interactions (see EPT/Polypharmacy/2022-08-30/Paper">ADR table)
- monitoring mechanisms for high-risk drugs
- risk of accidental overdosing
Identify adverse drug effects by checking for
- specific symptoms/laboratory markers (e.g. hypokalaemia)
- cumulative adverse drug effects (see EPT/Polypharmacy/2022-08-30/Paper">ADR table)
- drugs that may be used to treat side effects caused by other drugs
Medication Sick Day guidance
Person specific issues to address
- Advised regarding potential for adverse effects from multiple oral steroid courses. DEXA scan arranged. Inhaled corticosteroids treat the condition with reduced exposure to systemic effects, therefore reduced ADRs
- Risk of hypokalaemia with salbutamol over-use, Us and Es were normal
- Personalised Asthma Action Plan reinforces advice to take when symptoms of asthma control deteriorate
6. Sustainability
Is drug therapy cost-effective and environmentally sustainable?
Identify unnecessarily costly drug therapy by
- Consider more cost-effective alternatives (but balance against effectiveness, safety, convenience)
Consider the environmental impact
- Inhaler use
- Single use plastics
- Medicines waste
- Water pollution
Person specific issues to address
- MDI changed to DPI (Easyhaler®) due to inhaler technique, and discussed environmental impact of propellant gases in MDI compared to DPI
- Salbutamol DPI (Easyhaler®) has a dose counter, so will provide reassurance of medication availability, but with education and discussion about management of asthma to reinforce the importance of regular preventer therapy
7. Person-centredness
Is the person willing and able to take drug therapy as intended?
Does the person understand the outcomes of the review?
- Consider Teach back
Ensure drug therapy changes are tailored to individual’s preferences by
- Is the medication in a form they can take?
- Is the dosing schedule convenient?
- Consider what assistance they might have and when this is available
- Are they able to take medicines as intended
Agree and communicate plan
- Discuss with the individual/carer/welfare proxy therapeutic objectives and treatment priorities
- Agree with them what medicines have an effect of sufficient magnitude to consider continuation or discontinuation
- Inform relevant healthcare and social care carers, changes in treatments across the care interfaces Agreed plan
Person specific issues to address
Agreed plan
- Regular preventer therapy issued in an inhaler which they are able to use correctly
- Personalised Asthma Action Plan discussed and agreed, with a written copy given
- Discussed smoking cessation and Very Brief Advice (VBA) given. Considering referral to Quit Your Way
- Possible that a further referral to the Difficult Asthma Clinic may be needed, dependent on full results and outcomes from improved education and inhaler technique
- Review appointment made in 4 weeks
Contact
Email: EPandT@gov.scot
There is a problem
Thanks for your feedback